
Page 22 - SPEMD_61-2
P. 22
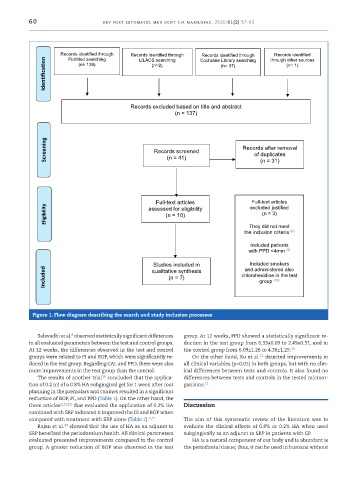
60 Figure 1 – Flow diagram describing the search and study inclusion processes.
rev port estomatol med dent cir maxilofac. 2020;61(2):57-63
Records identified through Records identified through Cochrane Library searching through other sources
Records identified
Records identified through
Identification (n= 138) (n=2) (n= 37) (n= 1)
PubMed searching
LILACS searching
Records excluded based on title and abstract
(n = 137)
Screening Records screened Records after removal
of duplicates
(n = 41)
(n = 31)
Full-text articles excluded justified
Full-text articles
Eligibility assessed for eligibility (n = 3)
(n = 10)
They did not meet
the inclusion criteria (8)
Included patients
with PPD <4mm
(9)
Included smokers
Studies included in and administered also
Included (n = 7) chlorohexidine in the test
qualitative synthesis
group
(10)
Figure 1. Flow diagram describing the search and study inclusion processes
8
Salavadhi et al. observed statistically significant differences group. At 12 weeks, PPD showed a statistically significant re-
in all evaluated parameters between the test and control groups. duction in the test group from 6.33±0.09 to 2.49±0.51, and in
At 12 weeks, the differences observed in the test and control the control group from 6.09±1.26 to 4.36±1.29. 13
11
groups were related to PI and BOP, which were significantly re- On the other hand, Xu et al. detected improvements in
duced in the test group. Regarding CAL and PPD, there were also all clinical variables (p<0.05) in both groups, but with no clin-
more improvements in the test group than the control. ical differences between tests and controls. It also found no
10
The results of another trial concluded that the applica- differences between tests and controls in the tested microor-
tion of 0.2 ml of a 0.8% HA subgingival gel for 1 week after root ganisms. 11
planning in the premolars and canines resulted in a significant
reduction of BOP, PI, and PPD (Table 1). On the other hand, the
three articles 2,11,13 that evaluated the application of 0.2% HA Discussion
combined with SRP indicated it improved the GI and BOP when
compared with treatment with SRP alone (Table 2). 2,11 The aim of this systematic review of the literature was to
13
Rajan et al. showed that the use of HA as an adjunct to evaluate the clinical effects of 0.8% or 0.2% HA when used
SRP benefited the periodontium health. All clinical parameters subgingivally as an adjunct to SRP in patients with CP.
evaluated presented improvements compared to the control HA is a natural component of our body and is abundant is
group. A greater reduction of BOP was observed in the test the periodontal tissue; thus, it can be used in humans without