
Page 17 - SPEMD_61-2
P. 17
rev port estomatol med dent cir maxilofac . 2020;61(2):52-56 55
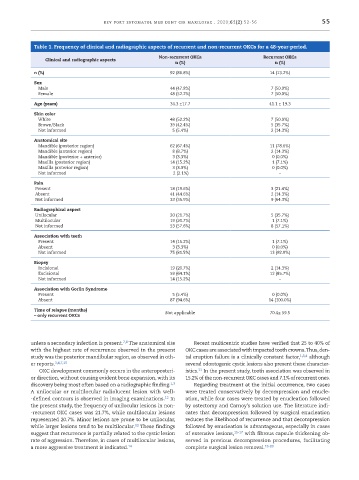
Table 1. Frequency of clinical and radiographic aspects of recurrent and non ‑recurrent OKCs for a 48 ‑year ‑period.
Non ‑recurrent OKCs Recurrent OKCs
Clinical and radiographic aspects
n (%) n (%)
n (%) 92 (86.8%) 14 (13.2%)
Sex
Male 44 (47.8%) 7 (50.0%)
Female 48 (52.2%) 7 (50.0%)
Age (years) 34.3 ±17.7 41.1 ± 19.3
Skin color
White 48 (52.2%) 7 (50.0%)
Brown/Black 39 (42.4%) 5 (35.7%)
Not informed 5 (5.4%) 2 (14.3%)
Anatomical site
Mandible (posterior region) 62 (67.4%) 11 (78.6%)
Mandible (anterior region) 8 (8.7%) 2 (14.3%)
Mandible (posterior + anterior) 3 (3.3%) 0 (0.0%)
Maxilla (posterior region) 14 (15.2%) 1 (7.1%)
Maxilla (anterior region) 3 (3.3%) 0 (0.0%)
Not informed 2 (2.1%) –
Pain
Present 18 (19.6%) 3 (21.4%)
Absent 41 (44.6%) 2 (14.3%)
Not informed 33 (35.9%) 9 (64.3%)
Radiographical aspect
Unilocular 20 (21.7%) 5 (35.7%)
Multilocular 19 (20.7%) 1 (7.1%)
Not informed 53 (57.6%) 8 (57.1%)
Association with teeth
Present 14 (15.2%) 1 (7.1%)
Absent 3 (3.3%) 0 (0.0%)
Not informed 75 (81.5%) 13 (92.9%)
Biopsy
Incisional 19 (20.7%) 2 (14.3%)
Excisional 59 (64.1%) 12 (85.7%)
Not informed 14 (15.2%) –
Association with Gorlin Syndrome
Present 5 (5.4%) 0 (0.0%)
Absent 87 (94.6%) 14 (100.0%)
Time of relapse (months) Not applicable 70.4± 59.5
– only recurrent OKCs
7,8
unless a secondary infection is present. The anatomical site Recent multicentric studies have verified that 25 to 40% of
with the highest rate of recurrence observed in the present OKC cases are associated with impacted tooth crowns. Thus, den-
study was the posterior mandibular region, as observed in oth- tal eruption failure is a clinically constant factor, 1,3,4 although
er reports. 3,4,7,10 several odontogenic cystic lesions also present these character-
11
OKC development commonly occurs in the anteroposteri- istics. In the present study, tooth association was observed in
or direction, without causing evident bone expansion, with its 15.2% of the non -recurrent OKC cases and 7.1% of recurrent ones.
1,3
discovery being most often based on a radiographic finding. Regarding treatment at the initial occurrence, two cases
A unilocular or multilocular radiolucent lesion with well- were treated conservatively by decompression and enucle-
-defined contours is observed in imaging examinations. In ation, while four cases were treated by enucleation followed
12
the present study, the frequency of unilocular lesions in non- by ostectomy and Carnoy’s solution use. The literature indi-
-recurrent OKC cases was 21.7%, while multilocular lesions cates that decompression followed by surgical enucleation
represented 20.7%. Minor lesions are prone to be unilocular, reduces the likelihood of recurrence and that decompression
while larger lesions tend to be multilocular. These findings followed by enucleation is advantageous, especially in cases
13
suggest that recurrence is partially related to the cystic lesion of extensive lesions, 15-17 with fibrous capsule thickening ob-
rate of aggression. Therefore, in cases of multilocular lesions, served in previous decompression procedures, facilitating
a more aggressive treatment is indicated. 14 complete surgical lesion removal. 18-20