
Page 43 - SPEMD_67-1
P. 43
rev port estomatol med dent cir maxilofac . 2026;67(1):34-39 37
in 10% neutral buffered formalin and submitted for histo-
pathological examination. Postoperative management includ-
ed ibuprofen 400 mg every 8 hours for 3 days and 0.12% chlor-
hexidine mouth rinse twice daily for 7 days; antibiotics were
not prescribed. The patient received instructions on oral hy-
giene and a soft diet during the initial healing period. The total
surgical time was approximately 35 minutes. Histopathologi-
cal analysis confirmed the diagnosis, and surgical margins
were reported as free of lesion.
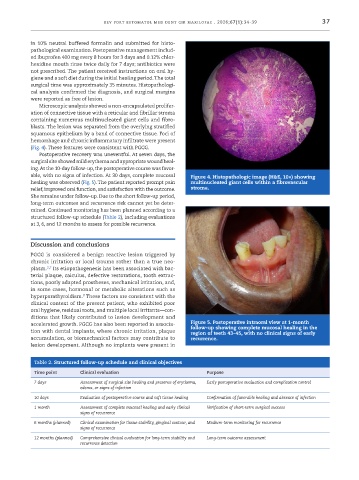
Microscopic analysis showed a non-encapsulated prolifer-
ation of connective tissue with a reticular and fibrillar stroma
containing numerous multinucleated giant cells and fibro-
blasts. The lesion was separated from the overlying stratified
squamous epithelium by a band of connective tissue. Foci of
hemorrhage and chronic inflammatory infiltrate were present
(Fig. 4). These features were consistent with PGCG.
Postoperative recovery was uneventful. At seven days, the
surgical site showed mild erythema and appropriate wound heal-
ing. At the 10-day follow-up, the postoperative course was favor-
able, with no signs of infection. At 30 days, complete mucosal Figure 4. Histopathologic image (H&E, 10×) showing
healing was observed (Fig. 5). The patient reported prompt pain multinucleated giant cells within a fibrovascular
relief, improved oral function, and satisfaction with the outcome. stroma.
She remains under follow-up. Due to the short follow-up period,
long-term outcomes and recurrence risk cannot yet be deter-
mined. Continued monitoring has been planned according to a
structured follow-up schedule (Table 2), including evaluations
at 3, 6, and 12 months to assess for possible recurrence.
Discussion and conclusions
PGCG is considered a benign reactive lesion triggered by
chronic irritation or local trauma rather than a true neo-
2,7
plasm. Its etiopathogenesis has been associated with bac-
terial plaque, calculus, defective restorations, tooth extrac-
tions, poorly adapted prostheses, mechanical irritation, and,
in some cases, hormonal or metabolic alterations such as
8
hyperparathyroidism. These factors are consistent with the
clinical context of the present patient, who exhibited poor
oral hygiene, residual roots, and multiple local irritants—con-
ditions that likely contributed to lesion development and
accelerated growth. PGCG has also been reported in associa- Figure 5. Postoperative intraoral view at 1-month
follow-up showing complete mucosal healing in the
tion with dental implants, where chronic irritation, plaque region of teeth 43–45, with no clinical signs of early
accumulation, or biomechanical factors may contribute to recurrence.
lesion development. Although no implants were present in
Table 2. Structured follow-up schedule and clinical objectives
Time point Clinical evaluation Purpose
7 days Assessment of surgical site healing and presence of erythema, Early postoperative evaluation and complication control
edema, or signs of infection
10 days Evaluation of postoperative course and soft tissue healing Confirmation of favorable healing and absence of infection
1 month Assessment of complete mucosal healing and early clinical Verification of short-term surgical success
signs of recurrence
6 months (planned) Clinical examination for tissue stability, gingival contour, and Medium-term monitoring for recurrence
signs of recurrence
12 months (planned) Comprehensive clinical evaluation for long-term stability and Long-term outcome assessment
recurrence detection