
Page 30 - SPEMD_60-4
P. 30
178 rev port estomatol med dent cir maxilofac. 2019;60(4):175-188
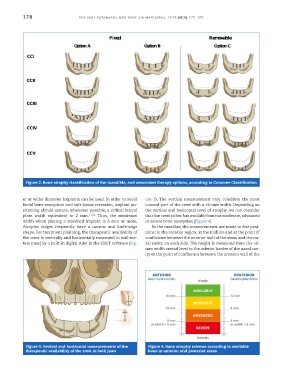
Figure 2. Bone atrophy classification of the mandible, and associated therapy options, according to Carames Classification
er or wider diameter implants can be used. In order to avoid ure 3). The vertical measurement only considers the most
facial bone resorption and soft-tissue recession, implant po- coronal part of the crest with a >6-mm width. Depending on
sitioning should ensure, whenever possible, a critical buccal the vertical and horizontal level of atrophy, we can consider
plate width equivalent to 2 mm. 31,32 Thus, the minimum that the crest either has available bone or moderate, advanced
width when placing a standard implant is 6 mm or more. or severe bone resorption (Figure 4).
Atrophic ridges frequently have a narrow and knife-edge In the maxillae, the measurements are made in five posi-
shape. For treatment planning, the therapeutic availability of tions: in the anterior region, at the midline and at the point of
the crest is vertically and horizontally measured in millime- confluence between the anterior wall of the sinus and the na-
ters (mm) by a built-in digital ruler in the CBCT software (Fig- sal cavity on each side. The height is measured from the >6-
mm width crestal level to the inferior border of the nasal cav-
ity or the point of confluence between the anterior wall of the
Figure 3. Vertical and horizontal measurements of the Figure 4. Bone atrophy scheme according to available
therapeutic availability of the crest in both jaws bone in anterior and posterior areas