
Page 59 - SPEMD_60-4
P. 59
rev port estomatol med dent cir maxilofac . 2019;60(4):205-209 207
prognosis. 1,2,27 The aim of this paper is to describe a clinical
case of a trichilemmoma in the perioral region, addressing the
clinical and histological characteristics that allowed its diag-
nosis, as well as review the treatment suggested in the litera-
ture for this pathology, in order to contribute to a greater
knowledge of this rare condition.
Case report
A 68-year-old male patient presented with an asymptomatic
lesion in his right lip commissure region after referral by his
oral hygienist for an oral medicine appointment. No relevant
medical history and no smoking or alcoholism were stated.
The patient was under treatment with simvastatin to control
hypercholesterolemia and pregabalin due to cervical spinal
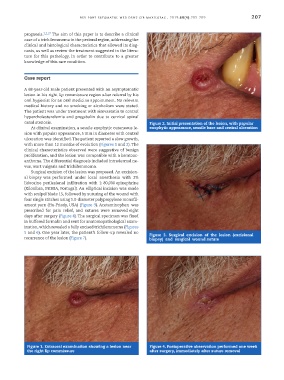
canal stenosis. Figure 2. Initial presentation of the lesion, with papular
At clinical examination, a sessile exophytic cutaneous le- exophytic appearance, sessile base and central ulceration
sion with papular appearance, 5 mm in diameter with central
ulceration was identified. The patient reported a slow growth,
with more than 12 months of evolution (Figures 1 and 2). The
clinical characteristics observed were suggestive of benign
proliferation, and the lesion was compatible with a keratoac-
anthoma. The differential diagnosis included intradermal ne-
vus, wart vulgaris and trichilemmoma.
Surgical excision of the lesion was proposed. An excision-
al biopsy was performed under local anesthesia with 2%
lidocaine perilesional infiltration with 1: 80,000 epinephrine
(Xilonibsa, INIBSA, Portugal). An elliptical incision was made
with scalpel blade 15, followed by suturing of the wound with
four single stitches using 5.0-diameter polypropylene monofil-
ament yarn (Hu-Friedy, USA) (Figure 3). Acetaminophen was
prescribed for pain relief, and sutures were removed eight
days after surgery (Figure 4). The surgical specimen was fixed
in buffered formalin and sent for anatomopathological exam-
ination, which revealed a fully excised trichilemmoma (Figures
5 and 6). One year later, the patient’s follow-up revealed no Figure 3. Surgical excision of the lesion (excisional
recurrence of the lesion (Figure 7). biopsy) and surgical wound suture
Figure 1. Extraoral examination showing a lesion near Figure 4. Postoperative observation performed one week
the right lip commissure after surgery, immediately after suture removal