
Page 35 - SPEMD_67-1
P. 35
rev port estomatol med dent cir maxilofac . 2026;67(1):27-33 29
Case 2
A 71-year-old male patient presented to the (placeholder for
the institution’s name), complaining of a lesion on the palate
with unknown duration. During the anamnesis, the medical
history was non-contributory, although the patient reported a
long-term habit of smoking and chewing tobacco. Extraoral
examination revealed no edema or facial asymmetry; howev-
er, the right submandibular lymph nodes were enlarged. In-
traoral examination revealed an extensive tumor mass located
on the palate, extending to the upper alveolar ridge and buccal
vestibule. The lesion presented exophytic growth, red-
dish-white coloration, and a cauliflower-like verrucous surface
(Figure 4). Therefore, the diagnostic hypothesis was VC. An in-
cisional biopsy was performed under local anesthesia, and the
specimen was sent for histopathological analysis.
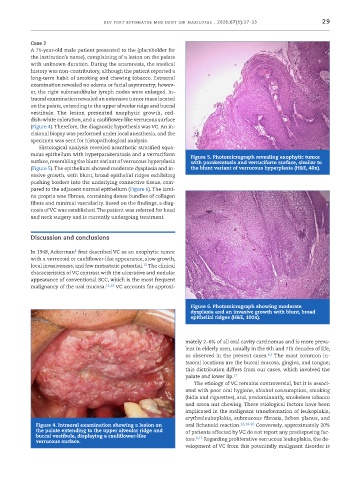
Histological analysis revealed acanthotic stratified squa-
mous epithelium with hyperparakeratosis and a verruciform Figure 5. Photomicrograph revealing exophytic tumor
surface, resembling the blunt variant of verrucous hyperplasia with parakeratosis and verruciform surface, similar to
(Figure 5). The epithelium showed moderate dysplasia and in- the blunt variant of verrucous hyperplasia (H&E, 40x).
vasive growth, with blunt, broad epithelial ridges exhibiting
pushing borders into the underlying connective tissue, com-
pared to the adjacent normal epithelium (Figure 6). The lami-
na propria was fibrous, containing dense bundles of collagen
fibers and minimal vascularity. Based on the findings, a diag-
nosis of VC was established. The patient was referred for head
and neck surgery and is currently undergoing treatment.
Discussion and conclusions
1
In 1948, Ackerman first described VC as an exophytic tumor
with a verrucoid or cauliflower-like appearance, slow growth,
15
local invasiveness, and low metastatic potential. The clinical
characteristics of VC contrast with the ulcerative and nodular
appearance of conventional SCC, which is the most frequent
malignancy of the oral mucosa. 15,16 VC accounts for approxi-
Figure 6. Photomicrograph showing moderate
dysplasia and an invasive growth with blunt, broad
epithelial ridges (H&E, 100x).
mately 2−6% of all oral cavity carcinomas and is more preva-
lent in elderly men, usually in the 6th and 7th decades of life,
as observed in the present cases. 6,7 The most common in-
traoral locations are the buccal mucosa, gingiva, and tongue;
this distribution differs from our cases, which involved the
palate and lower lip. 17
The etiology of VC remains controversial, but it is associ-
ated with poor oral hygiene, alcohol consumption, smoking
(bidis and cigarettes), and, predominantly, smokeless tobacco
and areca nut chewing. These etiological factors have been
implicated in the malignant transformation of leukoplakia,
erythroleukoplakia, submucous fibrosis, lichen planus, and
Figure 4. Intraoral examination showing a lesion on oral lichenoid reaction. 16,18-20 Conversely, approximately 20%
the palate extending to the upper alveolar ridge and of patients affected by VC do not report any predisposing fac-
buccal vestibule, displaying a cauliflower-like 6,15
verrucous surface. tors. Regarding proliferative verrucous leukoplakia, the de-
velopment of VC from this potentially malignant disorder is