
Page 29 - SPEMD_67-1
P. 29
rev port estomatol med dent cir maxilofac . 2026;67(1):21-26 23
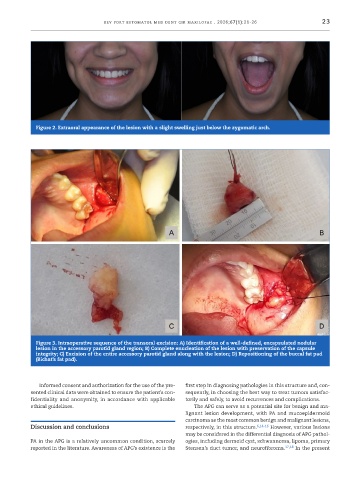
Figure 2. Extraoral appearance of the lesion with a slight swelling just below the zygomatic arch.
Figure 3. Intraoperative sequence of the transoral excision: A) Identification of a well-defined, encapsulated nodular
lesion in the accessory parotid gland region; B) Complete enucleation of the lesion with preservation of the capsule
integrity; C) Excision of the entire accessory parotid gland along with the lesion; D) Repositioning of the buccal fat pad
(Bichat’s fat pad).
Informed consent and authorization for the use of the pre- first step in diagnosing pathologies in this structure and, con-
sented clinical data were obtained to ensure the patient’s con- sequently, in choosing the best way to treat tumors satisfac-
fidentiality and anonymity, in accordance with applicable torily and safely, to avoid recurrences and complications.
ethical guidelines. The APG can serve as a potential site for benign and ma-
lignant lesion development, with PA and mucoepidermoid
carcinoma as the most common benign and malignant lesions,
Discussion and conclusions respectively, in this structure. 6,14-16 However, various lesions
may be considered in the differential diagnosis of APG pathol-
PA in the APG is a relatively uncommon condition, scarcely ogies, including dermoid cyst, schwannoma, lipoma, primary
reported in the literature. Awareness of APG’s existence is the Stensen’s duct tumor, and neurofibroma. 17,18 In the present