
Page 46 - SPEMD_62-3
P. 46
172 rev port estomatol med dent cir maxilofac. 2021;62(3):170-175
Although the patient did not remember to have suffered
a specific trauma in the face, he reported that this is a com-
mon happening in his daily sports practice. Based on the an-
amnesis and the clinical-radiographic aspect, the initial diag-
nostic hypothesis was that of a simple bilateral bone cyst, but
the possibility of other cystic lesions or odontogenic tumors
was not ruled out. Surgical exploration was suggested and an
informed consent form, which also contained an authoriza-
tion for the case report, was obtained from his mother. If the
surgery did not reveal empty bone cavities, an excisional bi-
opsy on the right side and incisional biopsy on the left side,
Figure 1. Panoramic radiograph showing well defined
bilateral radiolucent images in the mandible. with possible installation of a drain for decompression, was
planned.
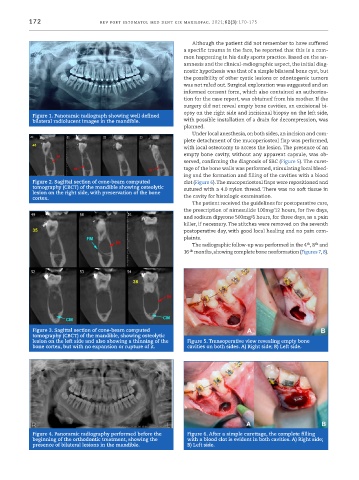
Under local anesthesia, on both sides, an incision and com-
plete detachment of the mucoperiosteal flap was performed,
with local osteotomy to access the lesion. The presence of an
empty bone cavity, without any apparent capsule, was ob-
served, confirming the diagnosis of SBC (Figure 5). The curet-
tage of the bone walls was performed, stimulating local bleed-
ing and the formation and filling of the cavities with a blood
Figure 2. Sagittal section of cone-beam computed clot (Figure 6). The mucoperiosteal flaps were repositioned and
tomography (CBCT) of the mandible showing osteolytic sutured with a 4.0 nylon thread. There was no soft tissue in
lesion on the right side, with preservation of the bone
cortex. the cavity for histologic examination.
The patient received the guidelines for postoperative care,
the prescription of nimesulide 100mg/12 hours, for five days,
and sodium dipyrone 500mg/6 hours, for three days, as a pain
killer, if necessary. The stitches were removed on the seventh
postoperative day, with good local healing and no pain com-
plaints.
th
th
The radiographic follow-up was performed in the 4 , 8 and
th
16 months, showing complete bone neoformation (Figures 7, 8).
Figure 3. Sagittal section of cone-beam computed
tomography (CBCT) of the mandible, showing osteolytic
lesion on the left side and also showing a thinning of the Figure 5. Transoperative view revealing empty bone
bone cortex, but with no expansion or rupture of it. cavities on both sides. A) Right side; B) Left side.
Figure 4. Panoramic radiography performed before the Figure 6. After a simple curettage, the complete filling
beginning of the orthodontic treatment, showing the with a blood clot is evident in both cavities. A) Right side;
presence of bilateral lesions in the mandible. B) Left side.