
Page 41 - SPEMD_62-3
P. 41
rev port estomatol med dent cir maxilofac . 2021;62(3):163-169 167
thin radiopaque halo and no root resorption or displacement
of the associated dental elements 13 and 15, despite bulging
of the cortical bone. The association with dental apices and
the indolent clinical -radiographic behavior of the COC led to
the clinical hypothesis of a radicular cyst.
The literature recommends enucleation associated with
lesion curettage, although marsupialization/decompression is
also among the treatments of choice for larger lesions to reduce
cyst size and surgery length. This maneuver has improved
22
prognosis, leading to low recurrence rates (approximately 5%).
In this report, due to the lesion’s size and well -circumscription,
enucleation associated with curettage was performed. The suc-
cess of this conservative treatment is evidenced by the lack of
recurrences in the last 3 years of follow -up.
COCs may be associated with other odontogenic lesions,
and the literature commonly reports association with odonto-
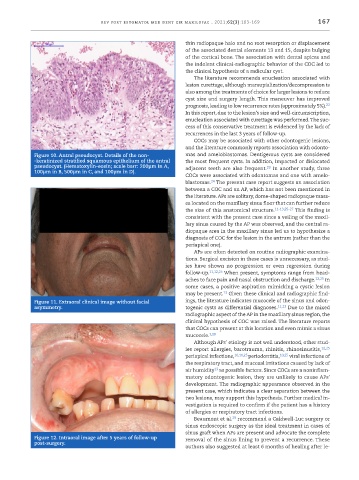
Figure 10. Antral pseudocyst. Details of the non- mas and ameloblastomas. Dentigerous cysts are considered
-keratinized stratified squamous epithelium of the antral the most frequent cysts. In addition, impacted or dislocated
pseudocyst. (Hematoxylin -eosin; scale barr: 200µm in A, adjacent teeth are also frequent. In another study, three
23
100µm in B, 500µm in C, and 100µm in D).
COCs were associated with odontomas and one with amelo-
24
blastomas. The present case report suggests an association
between a COC and an AP, which has not been mentioned in
the literature. APs are solitary, dome -shaped radiopaque mass-
es located on the maxillary sinus floor that can further reduce
the size of this anatomical structure. 11-13,25-27 This finding is
consistent with the present case since a veiling of the maxil-
lary sinus caused by the AP was observed, and the central ra-
diopaque area in the maxillary sinus led us to hypothesize a
diagnosis of COC for the lesion in the antrum (rather than the
periapical one).
APs are often detected on routine radiographic examina-
tions. Surgical excision in these cases is unnecessary, as stud-
ies have shown no progression or even regression during
follow -up. 11,12,25 When present, symptoms range from head-
aches to face pain and nasal obstruction and discharge. 12,25 In
some cases, a positive aspiration mimicking a cystic lesion
13
may be present. Given these clinical and radiographic find-
Figure 11. Extraoral clinical image without facial ings, the literature indicates mucocele of the sinus and odon-
asymmetry. togenic cysts as differential diagnoses. 11,13 Due to the mixed
radiographic aspect of the AP in the maxillary sinus region, the
clinical hypothesis of COC was raised. The literature reports
that COCs can present at this location and even mimic a sinus
mucocele. 3,28
Although APs’ etiology is not well understood, other stud-
ies report allergies, barotrauma, rhinitis, rhinosinusitis, 12,25
periapical infections, 10,11,25 periodontitis, 10,25 viral infections of
the respiratory tract, and mucosal irritations caused by lack of
air humidity as possible factors. Since COCs are a noninflam-
13
matory odontogenic lesion, they are unlikely to cause APs’
development. The radiographic appearance observed in the
present case, which indicates a clear separation between the
two lesions, may support this hypothesis. Further medical in-
vestigation is required to confirm if the patient has a history
of allergies or respiratory tract infections.
29
Beaumont et al. recommend a Caldwell -Luc surgery or
sinus endoscopic surgery as the ideal treatment in cases of
sinus graft when APs are present and advocate the complete
Figure 12. Intraoral image after 5 years of follow -up removal of the sinus lining to prevent a recurrence. These
post -surgery.
authors also suggested at least 6 months of healing after le-