
Page 40 - SPEMD_62-3
P. 40
166 rev port estomatol med dent cir maxilofac. 2021;62(3):163-169
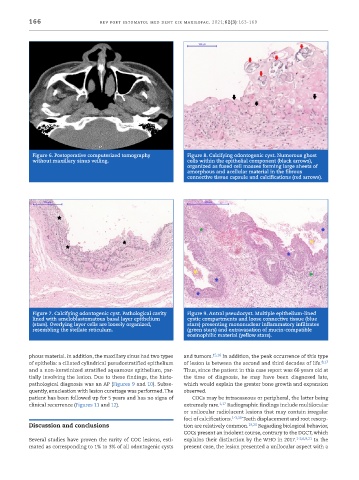
Figure 6. Postoperative computerized tomography Figure 8. Calcifying odontogenic cyst. Numerous ghost
without maxillary sinus veiling. cells within the epithelial component (black arrows),
organized as fused cell masses forming large sheets of
amorphous and acellular material in the fibrous
connective tissue capsule and calcifications (red arrows).
Figure 7. Calcifying odontogenic cyst. Pathological cavity Figure 9. Antral pseudocyst. Multiple epithelium -lined
lined with ameloblastomatous basal layer epithelium cystic compartments and loose connective tissue (blue
(stars). Overlying layer cells are loosely organized, stars) presenting mononuclear inflammatory infiltrates
resembling the stellate reticulum. (green stars) and extravasation of mucin -compatible
eosinophilic material (yellow stars).
phous material. In addition, the maxillary sinus had two types and tumors. 15,16 In addition, the peak occurrence of this type
of epithelia: a ciliated cylindrical pseudostratified epithelium of lesion is between the second and third decades of life. 8,17
and a non -keratinized stratified squamous epithelium, par- Thus, since the patient in this case report was 66 years old at
tially involving the lesion. Due to these findings, the histo- the time of diagnosis, he may have been diagnosed late,
pathological diagnosis was an AP (Figures 9 and 10). Subse- which would explain the greater bone growth and expansion
quently, enucleation with lesion curettage was performed. The observed.
patient has been followed up for 5 years and has no signs of COCs may be intraosseous or peripheral, the latter being
clinical recurrence (Figures 11 and 12). extremely rare. 1,17 Radiographic findings include multilocular
or unilocular radiolucent lesions that may contain irregular
foci of calcifications. 1-3,18 Teeth displacement and root resorp-
Discussion and conclusions tion are relatively common. 19,20 Regarding biological behavior,
COCs present an indolent course, contrary to the DGCT, which
Several studies have proven the rarity of COC lesions, esti- explains their distinction by the WHO in 2017. 1-2,6,8,21 In the
mated as corresponding to 1% to 3% of all odontogenic cysts present case, the lesion presented a unilocular aspect with a