
Page 39 - SPEMD_62-3
P. 39
rev port estomatol med dent cir maxilofac . 2021;62(3):163-169 165
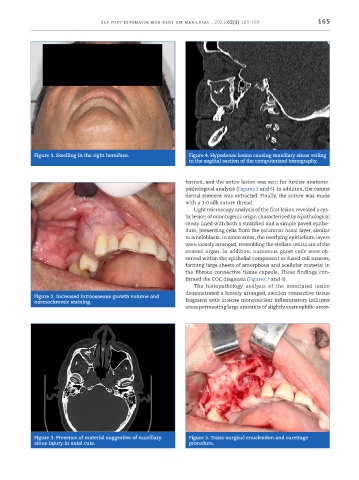
Figure 1. Swelling in the right hemiface. Figure 4. Hypodense lesion causing maxillary sinus veiling
in the sagittal section of the computerized tomography.
formed, and the entire lesion was sent for further anatomo-
pathological analysis (Figures 5 and 6). In addition, the canine
dental element was extracted. Finally, the suture was made
with a 3 -0 silk suture thread.
Light microscopy analysis of the first lesion revealed a cys-
tic lesion of odontogenic origin characterized by a pathological
cavity lined with both a stratified and a simple paved epithe-
lium, presenting cells from the columnar basal layer, similar
to ameloblasts. In some areas, the overlying epithelium layers
were loosely arranged, resembling the stellate reticulum of the
enamel organ. In addition, numerous ghost cells were ob-
served within the epithelial component as fused cell masses,
forming large sheets of amorphous and acellular material in
the fibrous connective tissue capsule. These findings con-
firmed the COC diagnosis (Figures 7 and 8).
The histopathology analysis of the associated lesion
demonstrated a loosely arranged, swollen connective tissue
Figure 2. Increased intraosseous growth volume and
normochromic staining. fragment with intense mononuclear inflammatory infiltrate
areas permeating large amounts of slightly eosinophilic amor-
Figure 3. Presence of material suggestive of maxillary Figure 5. Trans -surgical enucleation and curettage
sinus injury in axial cuts. procedure.