
Page 65 - SPEMD_62-1
P. 65
rev port estomatol med dent cir maxilofac . 2021;62(1):56-62 59
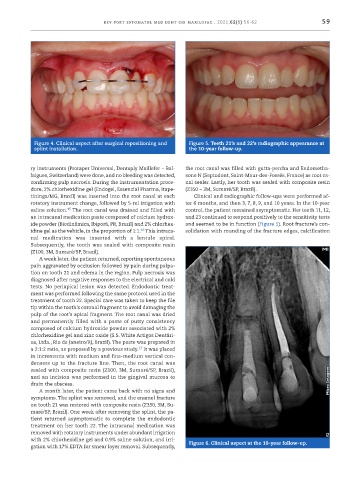
Figure 4. Clinical aspect after surgical repositioning and Figure 5. Teeth 21’s and 22’s radiographic appearance at
splint installation. the 10 -year follow -up.
ry instruments (Protaper Universal, Dentsply Maillefer – Bal- the root canal was filled with gutta -percha and Endometha-
laigues, Switzerland) were done, and no bleeding was detected, sone N (Septodont, Saint -Maur -des -Fossés, France) as root ca-
confirming pulp necrosis. During the instrumentation proce- nal sealer. Lastly, her tooth was sealed with composite resin
dure, 2% chlorhexidine gel (Endogel, Essencial Pharma, Itape- (Z350 – 3M, Sumaré/SP, Brazil).
tininga/MG, Brazil) was inserted into the root canal at each Clinical and radiographic follow -ups were performed af-
rotatory instrument change, followed by 5 -ml irrigation with ter 6 months, and then 3, 7, 8, 9, and 10 years. In the 10 -year
15
saline solution. The root canal was drained and filled with control, the patient remained asymptomatic. Her teeth 11, 12,
an intracanal medication paste composed of calcium hydrox- and 23 continued to respond positively to the sensitivity tests
ide powder (Biodinâmica, Ibiporã, PR, Brazil) and 2% chlorhex- and seemed to be in function (Figure 5). Root fracture’s con-
16
idine gel as the vehicle, in the proportion of 1:1. This intraca- solidation with rounding of the fracture edges, calcification
nal medication was inserted with a lentulo spiral.
Subsequently, the tooth was sealed with composite resin
(Z100, 3M, Sumaré/SP, Brazil).
A week later, the patient returned, reporting spontaneous
pain aggravated by occlusion followed by pain during palpa-
tion on tooth 21 and edema in the region. Pulp necrosis was
diagnosed after negative responses to the electrical and cold
tests. No periapical lesion was detected. Endodontic treat-
ment was performed following the same protocol used in the
treatment of tooth 22. Special care was taken to keep the file
tip within the tooth’s coronal fragment to avoid damaging the
pulp of the root’s apical fragment. The root canal was dried
and permanently filled with a paste of putty consistency
composed of calcium hydroxide powder associated with 2%
chlorhexidine gel and zinc oxide (S.S. White Artigos Dentári-
os, Ltda., Rio de Janeiro/RJ, Brazil). The paste was prepared in
17
a 2:1:2 ratio, as proposed by a previous study. It was placed
in increments with medium and fine -medium vertical con-
densers up to the fracture line. Then, the root canal was
sealed with composite resin (Z100, 3M, Sumaré/SP, Brazil),
and an incision was performed in the gingival mucosa to
drain the abscess.
A month later, the patient came back with no signs and
symptoms. The splint was removed, and the enamel fracture
on tooth 21 was restored with composite resin (Z350, 3M, Su-
maré/SP, Brazil). One week after removing the splint, the pa-
tient returned asymptomatic to complete the endodontic
treatment on her tooth 22. The intracanal medication was
removed with rotatory instruments under abundant irrigation
with 2% chlorhexidine gel and 0.9% saline solution, and irri- Figure 6. Clinical aspect at the 10 -year follow -up.
gation with 17% EDTA for smear layer removal. Subsequently,