
Page 58 - SPEMD_62-1
P. 58
52 rev port estomatol med dent cir maxilofac. 2021;62(1):50-55
General physical examination showed an asymptomatic the lesion was never mentioned and, on two occasions, had
firm mass on the left preauricular area, covered with normal received an antibiotic prescription alleging his discomfort was
skin (Figure 1). The intraoral examination did not reveal any due to the third molar removal.
abnormality. A panoramic radiograph and cone -beam tomography were
The patient presented his 2003, 2004, and 2013 panoramic requested and revealed an extensive radiolucent lesion ex-
radiographs, requested by different professionals, revealing tending from the retromolar area to the mandibular incisure,
the evolution of a large radiolucent lesion in the left posterior causing an expansion of the anterior border of the ramus and
ascending ramus (Figures 2, 3, and 4). The patient stated that perforation of the cortical bone (Figures 5 and 6). A routine
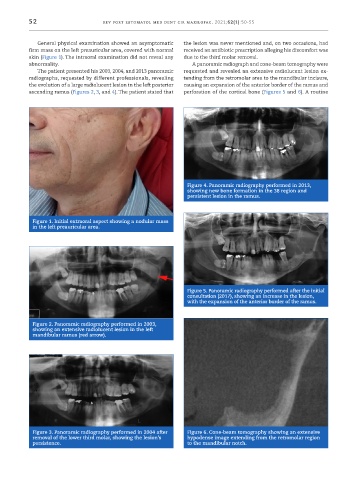
Figure 4. Panoramic radiography performed in 2013,
showing new bone formation in the 38 region and
persistent lesion in the ramus.
Figure 1. Initial extraoral aspect showing a nodular mass
in the left preauricular area.
Figure 5. Panoramic radiography performed after the initial
consultation (2017), showing an increase in the lesion,
with the expansion of the anterior border of the ramus.
Figure 2. Panoramic radiography performed in 2003,
showing an extensive radiolucent lesion in the left
mandibular ramus (red arrow).
Figure 3. Panoramic radiography performed in 2004 after Figure 6. Cone -beam tomography showing an extensive
removal of the lower third molar, showing the lesion’s hypodense image extending from the retromolar region
persistence. to the mandibular notch.