
Page 51 - SPEMD_62-1
P. 51
rev port estomatol med dent cir maxilofac . 2021;62(1):42-49 45
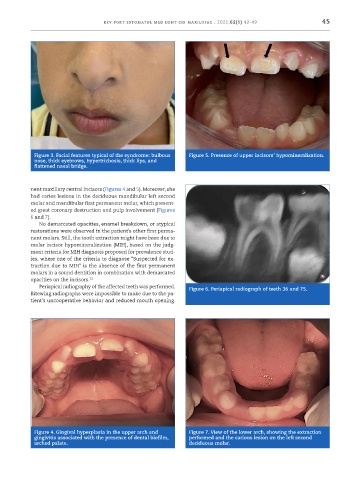
Figure 3. Facial features typical of the syndrome: bulbous Figure 5. Presence of upper incisors’ hypomineralization.
nose, thick eyebrows, hypertrichosis, thick lips, and
flattened nasal bridge.
nent maxillary central incisors (Figures 4 and 5). Moreover, she
had caries lesions in the deciduous mandibular left second
molar and mandibular first permanent molar, which present-
ed great coronary destruction and pulp involvement (Figures
6 and 7).
No demarcated opacities, enamel breakdown, or atypical
restorations were observed in the patient’s other first perma-
nent molars. Still, the tooth extraction might have been due to
molar incisor hypomineralization (MIH), based on the judg-
ment criteria for MIH diagnosis proposed for prevalence stud-
ies, where one of the criteria to diagnose “Suspected for ex-
traction due to MIH” is the absence of the first permanent
molars in a sound dentition in combination with demarcated
opacities on the incisors. 15
Periapical radiography of the affected teeth was performed. Figure 6. Periapical radiograph of teeth 36 and 75.
Bitewing radiographs were impossible to make due to the pa-
tient’s uncooperative behavior and reduced mouth opening.
Figure 4. Gingival hyperplasia in the upper arch and Figure 7. View of the lower arch, showing the extraction
gingivitis associated with the presence of dental biofilm, performed and the carious lesion on the left second
arched palate. deciduous molar.