
Page 61 - SPEMD_61-3
P. 61
rev port estomatol med dent cir maxilofac . 2020;61(3):148-153 151
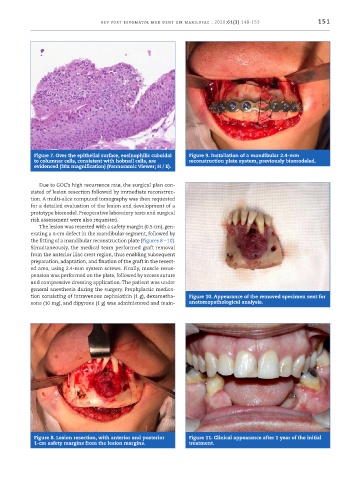
Figure 7. Over the epithelial surface, eosinophilic cuboidal Figure 9. Installation of a mandibular 2.4 -mm
to columnar cells, consistent with hobnail cells, are reconstruction plate system, previously biomodeled.
evidenced (30x magnification) (Pannoramic Viewer; H / E).
Due to GOC’s high recurrence rate, the surgical plan con-
sisted of lesion resection followed by immediate reconstruc-
tion. A multi -slice computed tomography was then requested
for a detailed evaluation of the lesion and development of a
prototype biomodel. Preoperative laboratory tests and surgical
risk assessment were also requested.
The lesion was resected with a safety margin (0.5 cm), gen-
erating a 4 -cm defect in the mandibular segment, followed by
the fitting of a mandibular reconstruction plate (Figures 8 – 10).
Simultaneously, the medical team performed graft removal
from the anterior iliac crest region, thus enabling subsequent
preparation, adaptation, and fixation of the graft in the resect-
ed area, using 2.4 -mm system screws. Finally, muscle resus-
pension was performed on the plate, followed by access suture
and compressive dressing application. The patient was under
general anesthesia during the surgery. Prophylactic medica-
tion consisting of intravenous cephalothin (1 g), dexametha- Figure 10. Appearance of the removed specimen sent for
sone (10 mg), and dipyrone (1 g) was administered and main- anatomopathological analysis.
Figure 8. Lesion resection, with anterior and posterior Figure 11. Clinical appearance after 1 year of the initial
1 -cm safety margins from the lesion margins. treatment.